An MCL injury usually occurs when a force strikes the outside of the knee. The MCL resists that force, and stretches or tears as a result. So what are the typical signs of a medial collateral ligament injury, and how do we treat it?
What is the medial collateral ligament?
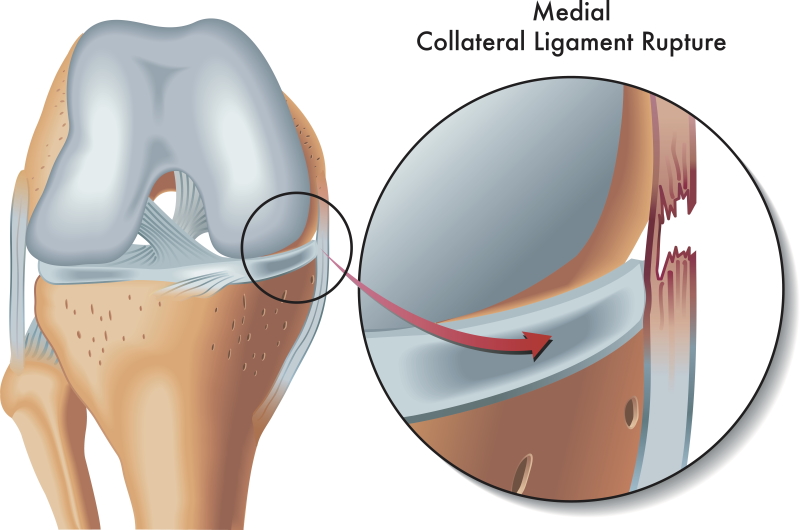
The MCL, or medial collateral ligament, is one of the four knee-stabilising ligaments. It’s a strong, fibrous band that runs from the end of the femur (thigh bone) to the top of the tibia (shin bone), on the inside of the knee. Its main job is to stop the knee opening up inwards. When the MCL tears completely, the knee becomes lax.
Most tears occur at the top, where the ligament attaches to the femur. Sometimes the tear happens at the lower attachment to the tibia — and these take longer to heal.
Diagnosis of an MCL injury

An MCL injury happens either on its own or alongside other ligament or cartilage injuries. The damage usually occurs during sport — bending, turning, or twisting — or from a direct blow to the outside of the knee that stretches and tears the ligament.
Typical symptoms of a medial collateral ligament injury include:
- Pain on the inside of the knee
- Localised swelling at the site of the tear
- A feeling of instability or buckling
- Difficulty fully bending or straightening the knee
We grade injuries by severity and by how loose the knee is on examination: a grade 1 injury has no laxity, a grade 2 is a partial tear with some laxity, and a grade 3 is a complete tear with significant laxity.
In some cases, an MRI confirms the MCL damage and rules out injury to other structures, such as the ACL or the meniscus.
MCL injury or meniscal injury: how can you tell?
An MCL injury usually occurs at the top attachment to the femur, so the pain and swelling sit above the joint line. A medial meniscal tear causes pain in the joint line, below the MCL’s top attachment, and can also cause general knee swelling, giving way, or locking. Telling them apart needs a careful examination.
ACL or MCL injury?
An ACL injury is usually more traumatic and more painful than an MCL injury. People often hear a pop or feel a tear, and the whole knee swells significantly. Examination shows laxity on specific ACL tests. The two can occur together, which is why a thorough assessment matters.
Treatment of an MCL injury

Treatment depends on the grade and severity.
We start with simple measures — regular ice, ibuprofen, and a compression sleeve. For grade 2 and 3 injuries, we add a hinged or limited-motion brace to protect the knee from side-to-side movement, sometimes restricting the range from 20 to 100 degrees to let the ligament heal. Braces are typically worn for 4–8 weeks, until stability and strength return.
Next, mobility exercises restore movement.
MCL sprain knee exercises
Rehabilitation then focuses on strength and balance before a return to sport. Compound exercises — weighted squats, lunges, deadlifts, incline leg press, and calf raises — rebuild knee strength. In the later stages, we progressively add more demanding tasks such as jogging, running, sprints, and side-to-side movements, which reduces the chance of re-injury.
Frequently asked questions about an MCL sprain knee
Is an MCL injection helpful?
We rarely use ultrasound-guided injections for MCL strains. Some doctors use PRP or dextrose to assist healing, but there’s no good evidence that an injection improves or speeds up recovery. Where we do inject, we use a high-concentration PRP system such as Arthrex ACP Max.
What is Pellegrini-Stieda syndrome (MCL calcification)?
Pellegrini-Stieda syndrome describes calcification of the MCL during healing, where calcium deposits form at its top attachment. X-ray or ultrasound detects them, and people often notice gradually worsening stiffness and pain during recovery. Treatment is usually ibuprofen and physiotherapy, and in some cases we use an ultrasound-guided cortisone injection to break up the calcium.
Is surgery an option for an MCL injury?
Usually not. Surgeons might consider it for a high-grade MCL injury combined with another ligament injury such as the ACL, a grade 3 injury in an elite athlete, or a tibial-sided tear where the ligament displaces above the pes anserine tendons (a Stener-type injury).
How long does an MCL sprain knee take to heal?
It depends on the grade: grade 1 takes 2–3 weeks, grade 2 around 6–8 weeks, and grade 3 up to 12 weeks. Your sport matters too — footballers often take longer, as side-to-side movements and kicking load the MCL. A tear near the lower (tibial) attachment often takes about twice as long as the more common upper tear.
What about an LCL injury — is it treated the same?
An LCL injury occurs when the knee bends outwards excessively, and it’s also graded by severity. The rehab is broadly similar, but with a few differences: the bracing differs, a grade 3 tear usually needs surgical repair or reconstruction, and LCL injuries are more often linked to other ligament or cartilage damage.
Final word from Sport Doctor London about an MCL injury
An MCL injury is one of the more common knee ligament injuries, and the great majority heal well without surgery. The key is grading it accurately, protecting it with the right bracing, and following a progressive rehabilitation programme — while excluding the ACL, meniscus, and other injuries that can occur alongside it.
If you have an inside-knee injury, Dr Masci can assess you in London, including ultrasound in clinic. Contact the team here or call +44 (0) 203 488 0350.
Leave A Comment